Caffeine, like other drugs and natural compounds, is metabolized by the cytochrome p450 (cyp450) pathway. It comprises several proteins that process several compounds such as the ones mentioned above. The easy way would be for all of us to have the same type of proteins, but this is unfortunately not the case! For instance, not everyone drives in the same way, right? Some like it fast, others not so much. Well, so the same thing happens to our proteins [1].
Cyp450 proteins work at three different speeds due to small changes in their “recipe” (i.e., there are polymorphisms). For each protein in this pathway, we have two different recipes: one from our father and another from our mother. Consequently, we can find different combinations of these proteins which usually work at three speeds (metabolizer phenotype): poor, normal, and ultra-rapid [1] . As shown in Figure 1, the speed of these proteins can be compared to the one reached by a tractor, a common car, or a formula one car.
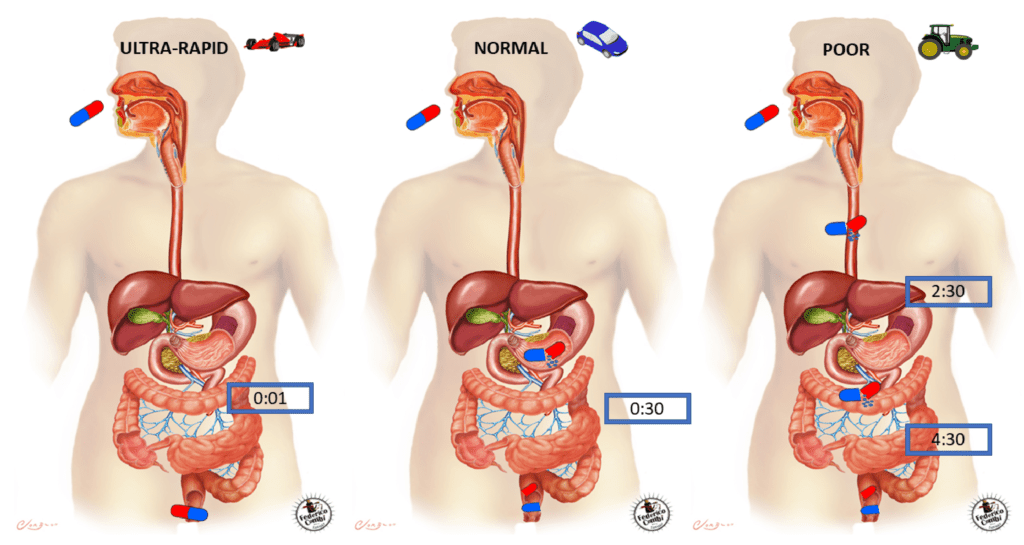
According to our proteins’ speed, we should not drink coffee after midday because they work at a slow pace (poor phenotype), and thus it is harder for them to metabolise caffeine (i.e., remove it from our system) before going to sleep. On the other hand, our proteins can remove the caffeine before it could even have its effect on us. In this case, if we drank water instead of coffee we would not even realize!
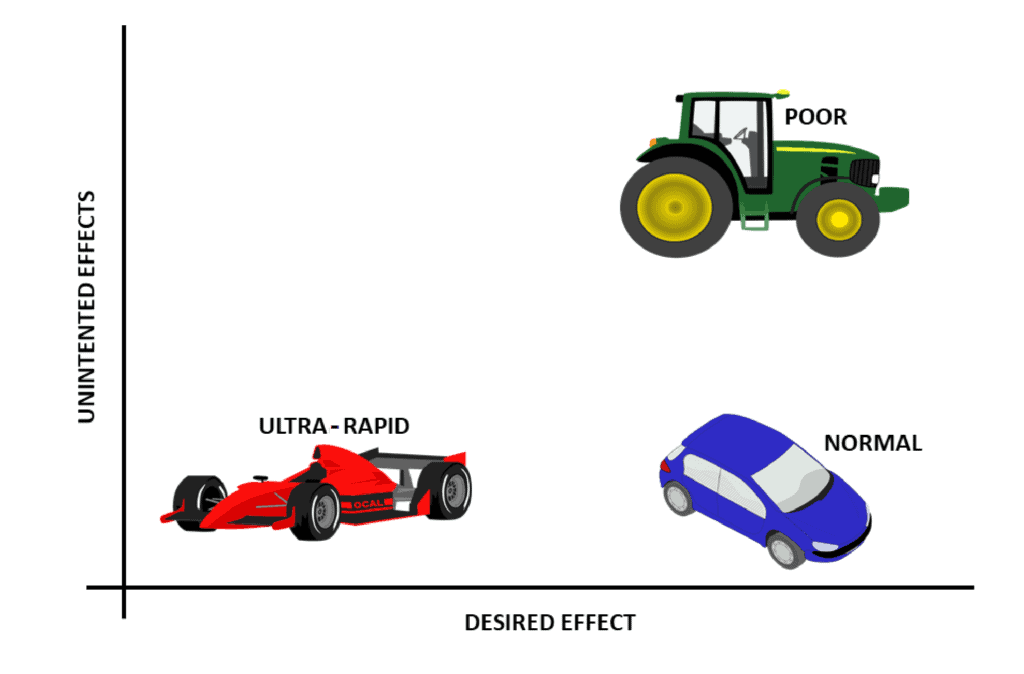
In addition, there are other factors that might affect our proteins’ speed (environmental interaction): we could be driving the fastest car (e.g., formula one car) but, if the road was packed, we would not be able to run, right? The cyp450 pathway works in the same fashion: if we take lots of drugs and/or natural substances that are metabolised by the proteins comprised in a specific metabolic pathway, we could overwhelm them, and thus things would work at a slower pace. This is one of the reasons why we should let our doctor know about all the drugs, chemicals, or natural compounds that we take so that they can personalise our treatment: we want to “avoid traffic jams” in our metabolic pathways. Bear in mind that the main goal of drugs is to make us feel better, even though sometimes their intake can cause side effects (see Figure 2). If our body has been exposed to specific drugs for a long time, they might eventually loose their effect on us or, what is worse, they might even trigger a harmful side effect. In other words, the drug could potentially damage our poor metabolizers (e.g., tractors). To avoid this situation, the results of a pharmacogenetic test could be helpful.
But wait… “pharma-what”? What does this word mean? Well, in a nutshell, a pharmacogenic test can measure our proteins’ speed in two ways. On the one hand, 24 hours after having ingested a specific compound, our urine can be analysed at a laboratory to measure how much of this compound has been secreted from our system. The quantity present in the urine is then correlated to the speed at which our proteins have been able to remove this compound. On the other hand, we could analyze the “recipe” of our proteins according to their changes and then extrapolate this to the theoretical speed at which our proteins might work.
In our lab, we analyze two genes (recipe) related to the cyp450 pathway. First, we read CYP3A5’s recipe. Specifically, when this protein does not work, we cannot activate a drug that has been administered to a patient to minimize transplant rejection, and thus it results in a higher risk of failure [2]. Furthermore, we also read CYP2D6’s recipe as this protein is needed as an oral treatment for a rare disease (Gaucher’s disease). Patients with “poor phenotypes” (e.g., tractors) need to reduce their drug intake to avoid harmful effects. Patients with “ultra-rapid phenotypes” (e.g., formula one), however, need another type of treatment as the drug ends up being ineffective for them [3].
Because of polytherapy, which is frequent in the elderly (whose grandpa does not take many pills, right?), pharmacogenetic studies are becoming more common. In addition, new complex drugs are being developed, which means that more monitoring is needed to measure how fast or how slow they carry out their roles in our bodies. Finally, other natural products such as valerian, green tea, or coffee are metabolised through the cyp450 pathway [4]; which means that doctors should consider how much of these natural compounds we take so they can personalize our treatment.
And… at the same time that I wrote this line, I finished my coffee! It may not have any effect whatsover on my system, but I do love its smell!
By Laura López de Frutos, @llopezdefrutos. Employee at Fundación Española para el Estudio y Terapéutica de la Enfermedad de Gaucher y otras lisosomales (FEETEG).
More information: