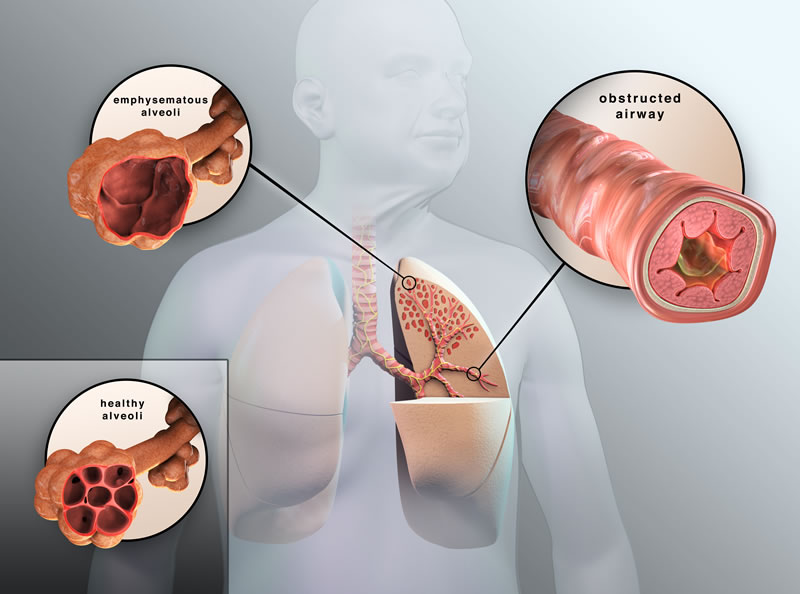
In 2015, 5% of the total deaths registered worldwide were due to a single disease, Chronic Obstructive Pulmonary Disease (COPD), a progressive and potentially fatal lung disease that may predispose to other respiratory diseases. It is important to note that COPD is preventable but not curable. According to the World Health Organization, in the year 2016 COPD prevalence reached 251 million. More than 90% of COPD deaths occur in developing countries.
To put this into perspective, COPD is the leading cause of death in Nepal, ahead of cardiovascular diseases, diabetes, and cancer. In that country, in the last twenty years, the incidence of COPD has doubled.
The main risk factor for COPD is exposure to tobacco smoke to both active and passive smokers. However, this is not the only cause: exposure to polluted air, such as in industrialized developing countries, is one of the main ones.

The symptoms of COPD are usually shortness of breath and chronic coughing with cough crises that, in addition to lasting up to weeks, may require hospitalization and lead to the death of the patient.
Despite the fact that COPD has no cure, both pharmacological and physiotherapy treatments relieve symptoms, improving patients’ quality of life and increasing their life expectancy.
COPD is currently diagnosed by measuring patients’ lung capacity. However, an early detection would greatly help to improve the quality of life of patients with this disease.
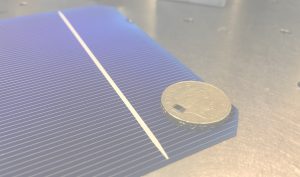
This is where the idea of the project that I am working on right now comes in, the miniaturization of an image technique widely known in medical diagnosis, Optical Coherence Tomography (OCT). OCT is based on the interference of two light beams. It has a tissue penetration of about three millimeters (depending on the tissue and the wavelength of the light used) with spatial resolution in the micrometers.
OCT is used as a diagnostic technique in several areas of medicine involving tissues that are easily accessible by light, such as ophthalmology where it is used to diagnose glaucoma (disease that causes progressive loss of vision) or also the vascular system. In the latter case, a probe is used to enter the arteries and diagnose cardiovascular diseases.
As in the case of the cardiovascular system, to diagnose COPD, a probe can be used. This probe is introduced through the trachea and down the respiratory bronchioles. However, the diameter of the target bronchioles is narrower than the available probes, for an early diagnosis. This means that using this technique for diagnosis, we discover the disease already in a fairly advanced state.
For that reason, the miniaturization of the technique is so important. In the project I am working on right now, we are integrating all the components of the OCT interferometer in a silicon chip, such as those used in telecommunications, with a size smaller than one millimeter and that would therefore be able to reach the narrowest diameter bronchioles, thus accelerating the diagnosis of COPD.
Among the challenges we face in the project are the integration of the light source into the chip itself, building 3D images with a chip with no moving parts, or getting the signal out of the lung to reconstruct the images in a computer.
Our goal is, as in the film of our childhood, in some way, to shrink the doctor to get a diagnostic tool that is cheaper, faster and, less intrusive for the patient. In addition, as the device in which we work is of a very small size, it is easily transportable, ensuring that patients do not have to travel to a hospital. Thanks to this device, it could be the doctor themself who goes to remote locations to diagnose people whose circumstances make it impossible to travel to a hospital, as could be the case in mountainous areas of Nepal.
In our project we still have a lot of work to do to achieve our goal, however, we will not rest until we have it; we scientists, we are sometimes very stubborn.
More information:
https://www.who.int/es/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd)
Mathers CD, Loncar D (November 2006). “Projections of global mortality and burden of disease from 2002 to 2030”. PLoS Medicine. 3 (11): e442.
Roleder T, et al. (2015) The basics of intravascular optical coherence tomography. Postępy w Kardiologii Interwencyjnej = Advances in Interventional Cardiology 11(2):74-83.
Post by Dr Laura Martínez Maestro, Postdoctoral Research Associate at the University of Manchester, Northwest SRUK constituency.